How does the procedure work?
You will have a local anaesthetic for the procedure. The angioplasty and stenting procedure will last around an hour and tends to be performed as an out-patient procedure, though in some cases patients are admitted to hospital overnight afterwards.
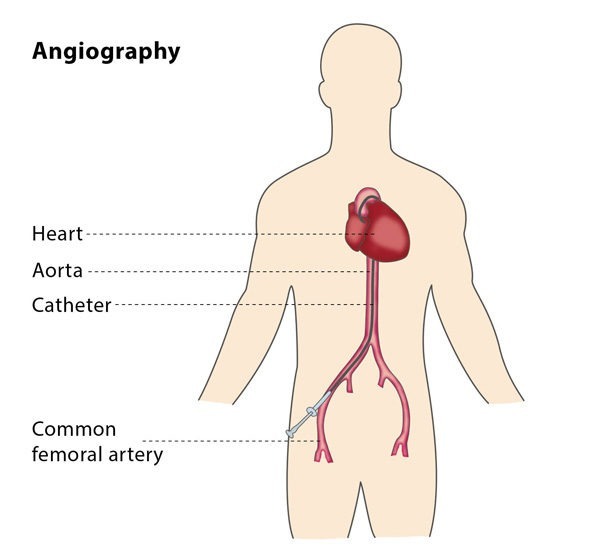
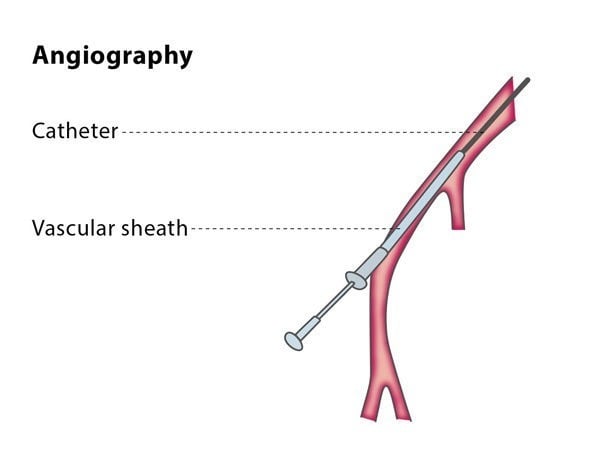
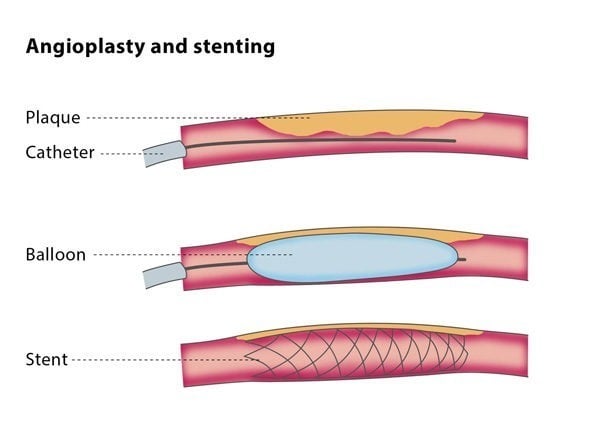
The interventional radiologist will puncture an artery in your thigh with a small needle and will then thread a combination of plastic tubes (called sheaths and catheters) into your arteries. Throughout the procedure, the interventional radiologist will use imaging for guidance. A balloon catheter will be inflated across the narrowed or obstructed part of the vessel; you may experience some discomfort at this point. In some cases, the balloon angioplasty is enough to keep the vessel open, but in other cases the vessel needs more support, so a stent is placed. This means the interventional radiologist will put a stent into the vessel to ensure it stays open.
Your vital signs will be monitored during and after the procedure, and you may be able to eat a light meal later the same day.
Why perform it?
This procedure may be beneficial for you if you suffer from leg pain when walking (intermittent claudication) or if you have a restricted blood supply in your legs (leg ischaemia) as a result of diabetes. The angioplasty and stenting procedure can also be a treatment for peripheral arterial disease and for narrowed or blocked arteries in your kidneys.
Angioplasty and stenting is a way to restore blood flow, relieve pain caused by restricted blood flow, improve kidney function and protect the brain from strokes.
What are the risks?
The success rate of the procedure is usually around 90-95%, though it varies according to the extent and complexity of the blockages in the artery. The majority of patients experience significant clinical improvement, meaning that their pain decreases and any wounds in the area heal better.
In around 10-15% of cases (the rate depends on the location and particular structure of the artery), the affected artery becomes blocked again, known as restenosis. If this happens to you, your symptoms will return and you will need to be treated again.
Minor complications are unusual but include bleeding, bruising and infection. In rare cases, patients have an abdominal haemorrhage, which requires a stay in hospital and patients may need blood transfusions. It is possible that the artery will be damaged by the balloon, causing the vessel to rupture, in which case the interventional radiologist will place a covered stent in the vessel to control any bleeding. The balloon inflation may cause small fragments from the blockage to break off and block other smaller vessels, causing the blood flow to be restricted even more. There is a very low risk of losing a limb or stroke, depending on the location of the artery on which the procedure is carried out.
Although the interventional radiologist will do all they can do minimise the risk of an allergic reaction, there is a risk of a reaction to the dye used in the imaging technique.
Bibliography
1. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG; TASC II Working Group, Bell K, Caporusso J, Durand-Zaleski I, Komori K, Lammer J, Liapis C, Novo S, Razavi M, Robbs J, Schaper N, Shigematsu H, Sapoval M, White C, White J, Clement D, Creager M, Jaff M, Mohler E 3rd, Rutherford RB, Sheehan P, Sillesen H, Rosenfield K. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg. 2007; 33 Suppl 1:S1-75.
2. Rooke TW, Hirsch AT, Misra S, Sidawy AN, Beckman JA, Findeiss L, Golzarian J, Gornik HL, Jaff MR, Moneta GL, Olin JW, Stanley JC, White CJ, White JV, Zierler RE; American College of Cardiology Foundation Task Force; American Heart Association Task Force. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013 Apr 9; 61(14):1555-70. doi: 10.1016/j.jacc.2013.01.004.